The ACP Billing Code Trap: Why Your Advance Care Planning Program May Be Failing Your Patients—and Your Bottom Line
January 28, 2026

You’re seeing the billing codes come through. Your providers are documenting ACP conversations. The boxes are getting checked.
But here’s the uncomfortable question: Is any of it actually working?
A recent analysis of Medicare claims data from an accountable care organization tells a troubling story—one that should give every ACO and health plan leader pause before assuming their advance care planning efforts are paying off.
The Numbers That Should Keep You Up at Night
In this analysis, 35% of patients who died within the past year had been billed for an advance care planning service at some point. On paper, that looks like progress. ACP conversations are happening. Documentation exists. Providers are engaging.
But dig one layer deeper and the picture falls apart.
Of all the patients who had an ACP billing event, 67% either never utilized hospice or entered hospice in the final seven days of life. These patients—the ones with documented ACP—accounted for nearly a third of total end-of-life costs in the analysis, while representing just 23% of the population.
And here’s the number that really stings: patients with ACP billing spent 73% more in their final year of life than those without.
Read that again. The patients your organization billed for ACP conversations had significantly higher costs than those who never had a documented ACP event at all.
What’s Actually Going On Here?
This isn’t an argument against advance care planning. The evidence is overwhelming that meaningful ACP—when done well—reduces unwanted aggressive interventions, increases hospice utilization, improves family satisfaction, and lowers costs.
The problem is that billing for ACP and actually doing effective ACP are two very different things.
A billing code captures that a conversation happened. It doesn’t capture whether that conversation was meaningful. It doesn’t tell you if the patient actually understood their options. It doesn’t indicate whether preferences were documented in a way that travels with the patient. And it certainly doesn’t guarantee that those preferences will be honored when it matters most.
What we’re likely seeing in this data is a combination of factors:
Checkbox ACP. The conversation happened because it was supposed to happen—during an AWV, because quality metrics require it, because the EHR prompted it. But the conversation was rushed, surface-level, or focused on paperwork completion rather than genuine values exploration.
Disconnected documentation. An advance directive might exist somewhere, but it’s not integrated into clinical workflows. When a patient shows up in the ED at 2 AM, no one can find it. Or worse, no one looks.
No follow-through. ACP isn’t a one-time event. Preferences change. Health status changes. A single conversation three years ago doesn’t help when a patient is facing a serious illness diagnosis today.
Wrong timing. The average time between ACP billing and death in this analysis was roughly 300 days. That sounds reasonable—but if the conversation happened during a routine visit when the patient was relatively healthy, it may not have addressed the realities they’d face at end of life.
The Hospice Connection
The data tells another story worth examining. Only 6% of patients in this analysis enrolled in hospice 3-12 months before death—the window that research suggests leads to the best outcomes for patients and families. Meanwhile, 63% either never enrolled in hospice or enrolled in the final week of life.
Patients who enrolled in hospice during that optimal 3-12 month window had substantially lower end-of-life costs. This isn’t surprising. Hospice replaces high-cost acute interventions with comfort-focused care that aligns with what most patients say they want when asked.
But here’s the connection that matters: effective advance care planning should lead to timely hospice enrollment. If your ACP program is working, you should see patients choosing hospice earlier—not in a crisis, not in the final days, but when it can actually provide the support patients and families need.
If you’re seeing ACP billing codes but not seeing movement in hospice utilization patterns, that’s a red flag. The conversations aren’t translating into action.
What Should You Be Measuring Instead?
Billing codes are easy to count. Outcomes are harder—but they’re what actually matter.
If you want to know whether your ACP program is working, look at:
Hospice utilization rates and timing. What percentage of your decedents used hospice? What was their average and median length of stay? Are you seeing improvement over time?
Terminal hospitalization rates. How many patients are dying in the hospital? In the ICU? These are often indicators of care that didn’t align with patient preferences.
Advance directive accessibility. When a patient arrives in a clinical setting, can providers actually find and access their documented preferences? How often does this happen?
Surrogate decision-maker engagement. Does the designated healthcare agent actually know they’ve been named? Do they understand the patient’s wishes? Have they been part of the conversation?
Patient and family experience. After a death, do families feel the care their loved one received aligned with what they would have wanted?
The Path Forward
None of this means you should stop billing for ACP. It means you should stop assuming the billing code equals success.
Effective advance care planning requires intentional design. It requires meeting patients where they are—not just during an annual wellness visit, but when they’re facing a new diagnosis, a hospitalization, a transition in care. It requires documentation that’s accessible and actionable. It requires follow-up and iteration as circumstances change.
And increasingly, it requires dedicated resources. Asking already-stretched primary care providers to have deep, meaningful conversations about values and end-of-life preferences during a 15-minute visit isn’t realistic. Organizations that are seeing real results are investing in specialized support—whether that’s trained care navigators, palliative care teams, or technology platforms designed specifically for this purpose.
The opportunity is real. Patients who receive quality advance care planning have better experiences. Families have less burden and regret. And yes, costs come down—not through rationing, but through aligning care with what patients actually want.
But you won’t get there by counting billing codes.
Summary of Findings: Medicare ACP Billing Code Analysis (ACO Claims Data)
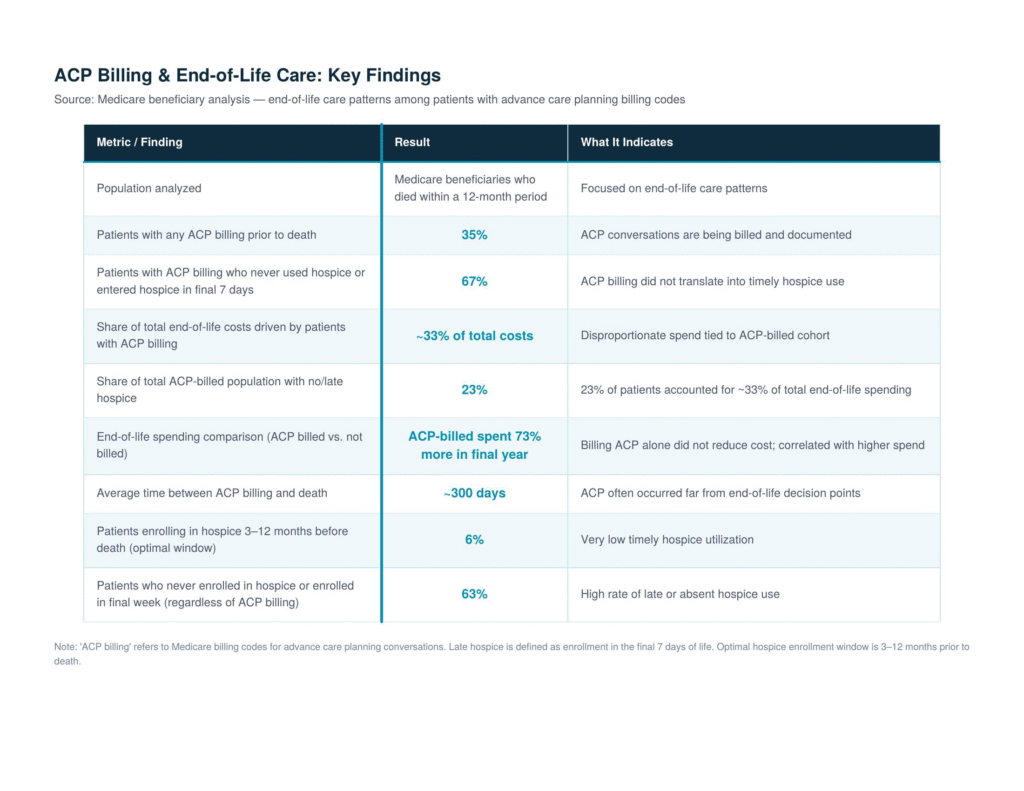 Table (1)
Table (1)The data referenced in this article comes from an analysis of Medicare claims data from an accountable care organization, examining end-of-life costs and care patterns for patients who died within a 12-month period.

")

